
Short Communication / Open Access
DOI: 10.31488 /bjhd.111
What Physical Activities can be Recommended in Cardiac Rehabilitation Centers?
DUC Philippe*1, ILIOU Marie-Christine2, AUMONT Marie-Claude1, CARBONNIER Antoine1, PARPAILLON Julie1, Michel Komajda1, Romain Cador1
1. Department of Cardiology, Groupe Hospitalier Saint-Joseph, Paris, 189 rue Raymond Losserand, 75014 Paris, France
2. Cardiac rehabilitation center, Corentin Celton Hospital, 4 Parvis Corentin Celton, 92130 Issy les Moulineaux, France
*Corresponding author: Philippe DUC, Réadaptation cardiaque, Groupe Hospitalier Saint-Joseph, Paris, 189 rue Raymond Losserand, 75014 Paris, France, 33 1 44 12 63 47, mobile 33 6 64 54 37 04, pduc@ghpsj.fr
Abstract
The physical activities practiced during a cardiac rehabilitation program are mainly based on ergometers or treadmill. Several other activities have been studied for coronary artery disease or congestive heart failure. Tai chi was studied in congestive heart failure but did not show a significant improvement for peak V02 even though beneficial effects were observed for the quality of life, the 6 min walk test, the level of BNP. Yoga life-style program has been studied after coronary artery by pass surgery, it improved significantly left ventricle ejection fraction and secondary outcomes (body mass index, lipid profile in particular a reduction in LDL), psychological variables with a significant improvement in different questionnaires of quality of life, Hospital anxiety and depression (HADS) –anxiety, HADS-depression , perceived stress scale (PSS) and positive and negative affect scale (PANAS)-negative. Yoga showed beneficial effects of yoga in relevant end-points in particular for the management of risk factors. Walking football adapted to patients has been proposed but not in cardiac rehabilitation centers and limited data are available with beneficial effects on secondary end-points (body fat mass, reduced percentage body fat and an increase in time of volutional exhaustion.Waltz dance showed beneficial effects on V02, VE/VC02 slope, V02/W slope, endothelium-dependant relaxation, HDL and triglycerides ejection fraction measured by echocardiography and the quality of life (Minessota heart failure living questionnaire MHFLQ, NYHA class). Nordic walking was tested as an alternative in heart failure patients . Telehealth exercise seems as effective as in rehabilitation centers but future studies needed to be performed to determine the beneficial effects. Even if biking and running are the main activities there is a vast field of research for additionnal or alternatives physical activities.
Keywords : Cardiac rehabilitation, tai chi, yoga, waltz dance
Introduction
Cardiac rehabilitation after acute coronary syndrome decreases recurrent myocardial infarction and mortality, improves quality of life, wellbeing and cardiorespiratory fitness [1,2] and in congestive heart failure (CHF) improves quality of life, cardiorespiratory fitness, decrease hospital readmission with an uncertain effect on mortality [3,4]. For several decades cardiac rehabilitation is part of the European and American guidelines in coronary and CHF [5,6] even though only a minority of patients from 10 to 30 % have an access to cardiac rehabilitation with multiple barriers for this low percentage [7].
Several components are part of a cardiac rehabilitation program : treatments optimization, correction of cardiovascular risk factors, therapeutic education and physical activities [8,9]. For exercise training the two main classical activities are based on biking and running (cyclo-ergometers and/or treadmill) with various protocols [10,11].
However, other type of physical activities, among which some more pleasant and so more able to increase the sustainability have been proposed as efficient alternatives. This review summarizes the effects of these alternatives in cardiac rehabilitation centers.
Tai chi has been studied in a randomized study [12] in heart failure (HF) patients comparing tai chi twice a week in a center and recommended three times/week at home versus a control groupe wit a classical rehabilitation. The patients had an average age of 64 ± 13 year, left ventricular ejection fraction (LVEF) of 23 ± 7%, an average class II of NYHA. At the end of the 12 week study there was a non significant improvement of the primary end point of the peak of V02 in the tai-chi group (10.5 ± 3 then 11.4 ± 3 versus 11.1 ± 6 then 10.4 ± 6 in the control group, P = 0.08, figure 1. Inversely there was a statistical improvement for the quality of life assessed with the Minnesota Living with heart failure (-25 points), an increase of the 6 min walk test (135 m, P = 0,001), a decrease of the natriuretic peptides (BNP – 138 pg/ml, p=003, table 1). It has to be noticed that there were only 15 patients in each group, that the tai chi method included slow motion movements corresponding to a moderate physical activity of 2-4 Mets and meditation. These elements may explain the non-statistical improvement of the primary end-point. Interestingly as that all secondary end-points showed benefits with tai chi this activity might be relevant or an alternative in some patients for whom running or biking is awkward.
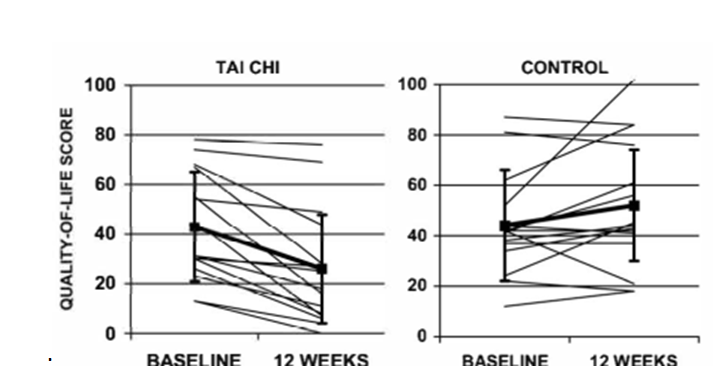
Figure 1.Change in peak oxygen uptake from baseline to 12 weeks. Means (± SD) are shown in bold. At 12 weeks, there was no significant difference between the two groups (p = 0.08) from [12]
Yoga has been studied in several studies. After coronary artery bypass in a randomized clinical trial with 250 male aged 35-65 year old, LVEF > 30%, it has been shown an improvement in ejection fraction, lipidic profile and anxiety [13]. The yoga protocol consisted in physical exercices, mental and emotionnal exercices to reach a control of mind modification based on yoga Chitta Vritti Nirodhah through “effortless blissful inner awarenesss”. Yoga life style program improved significantly left ventricle ejection fraction at 6 week, 6 month and 1 year and secondary outcomes : body mass index (p<0.001), lipid profile in particular a reduction in LDL (p=0.001 compared to control p=0.03), psychological variables with a significant improvement in different questionnaires of quality of life: HADS –anxiety (p=0.001), HADS-depression (p=0.001), PSS (p=0.001) and PANAS-negative (p=0.003) table 2.
Another large randomized study including 3,959 patients after acute coronary syndrome was conducted in 24 medical centers in India [14]. The patients were randomized between an enhanced standard of care involving educational program and a Yoga-Care program. The yoga–care program involved 13 sessions over 12 weeks with gentle yoga exercises followed by discussions to improve lifestyle and psychosocial concerns.
The co-primary outcomes were 1/ first occurrence of major adverse cardiovascular events (MACE) composite of all-cause mortality, myocardial infarction, stroke or emergency cardiovascular hospitalization and 2/self-rated health on the European quality of life-5 dimensions-5 level visual analogue scale at 12 weeks. The mean age was 53.4 ± 10.9 years, 14% of women, the follow-up was of 21.6 months. The MACE occurred in 6.7 % (131) patients in the Yoga-Care group and 7.4 % (146) patients in the enhanced standard care group (HR 0.9, 95 CI 0.71-1.15, p=0.41, figure 2) Self-rated health was 77 in the yoga-Care group and 75.7 in the other group (Figure 2).
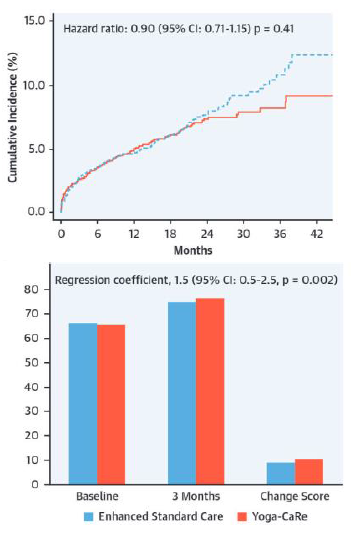
Figure 2.Yoga-Care versus enhanced standard care on major cardiovascular events from [14].
Coprimary outcome :
1. Major adverse cardiovascular events , Cumulative incidence of major cardiovascular events (composite death, nonfatal myocardial infarction, nonfatal stroke or emergency cardiovascular hospitalization).
2. Coprimary outcome : self-rated health (EQ-VAS Score)
Th return to pre-infarct activities score (reintegration to normal living index) at 12 week was 88.3 in the yoga-care group and 87.0 in the enhanced standard care group (difference in meann in favor of yoga-care group: 1.3, 95% CI 0.06-2.54, p=0.039). No difference in serious adverse events was reported between the two groups.
The specificity of the yoga-care program was that instead of having intense aerobic exercice it consisted in breathing movements, meditation, stretching movements. These low level activities stimulate parasympathetic nervous system, reduced downstream vascular and endocrine effets, increase in serotonin and decrease in dopamine [15-17].
This trial is the first large study showing that yoga was safe and effective in improving quality of life, return to pre-infarct activities after myocardial infarction. There was less major adverse cardiovascular in the yoga group but the study lacked statistical power to show a difference due to a lower rate of events than expected.
Football adapted to patients has been proposed in a less physical demanding efforts in a walking form [18] and studied in a 12 week study where it has been showed a benefical effect on body fat mass, reduced percentage body fat and an increase in time of volutional exhaustion [19]. However these studies were not performed during a cardiac rehabilitation and the intensity of exercice and the number of patients were limited.
Telehealth exercise seems as effective as in rehabilitation centers [20] and future studies needed to be performed to determine how physical activities in centers can be prolonged or coordinated with telehealth.
Physical activities are a core component of a cardiac rehabilitation program and biking and running are the main physical activities. Apart of these two activities additionnal activites may be added but a lack of knowledge and ressources for instance for yoga limit their widespread use.
As that one of the failure of lifestyle is the lack of maintenance of physical activity after a cardiac rehabilitation programm it was attractive to study a widespread activity like dancing. Waltz dance was studied in a randomized study by Belardinelli [21]. The patients were randomized between a classical rehabilitation programm and waltz dance practiced three times a week for 8 weeks at a level of 70% of peak of V02. The sequence of waltz was 5 minutes of slow waltz, 3 minutes of fast waltz, 5 minutes slow, 3 minutes fast, and 5 minutes slow for a total of 21 minutes. At the completion of the study period V02, VE/VC02 slope, V02/W slope, endothelium-dependant relaxation, HDL and triglycerides were improved signicantly in both groups but there was no statistical difference between the two groups for ejection fraction measured by echocardiography. The MHFLQ and NYHA class improved significantly in both groups (p< 0.001) but did not differ significantly between groups.
This study showed that waltz dancing was as effective as the classical aerobic exercice for the parameters used to assess the benefit of a cardiac rehabilitation programm (Table3). There was a higher adherence with dancing than with traditional exercice training. Waltz dancing or other dances can be proposed to be added or replaced the traditional exercices in a cardiac rehabilitation center.
There are data showing benefits of alternative activities to biking an running: tai chi, yoga, waltz dancing and potentially walking football. These alternative activities may replace biking and runing and can help to improve adherence to a cardiac rehabilitation program and improve physical activities after cardiac sessions.
Table 1:Comparison of the effects of Tai Chi versus usual care only on changes in outcomes during the 12-week trial, from [12].
| Tai Chi (n = 15) | Control (n = 15) | |||||
|---|---|---|---|---|---|---|
| Outcome measure | Baseline | 12 week | Baseline | 12 week | Between-group Difference in change | P value |
| Minnesota living with Heart Failure score | 43 ± 21 | 26 ± 23 | 44 ± 20 | 52 ± 25 | -25 (-36 to -14) | 0.001 |
| 6-min walk test (m) | 327 ± 106 | 412 ± 116 | 340 ± 117 | 289 ± 165 | + 135 (85 to 185) | 0.001 |
| Serum B-type natriuretic peptide (pg/ml) | 329 ± 377 | 281 ± 365 | 285 ± 340 | 375 ± 429 | -138 (-257 to – 9) | 0.03 |
| Plasma norepinephrine (ng/ml) | 1.3 ± 0.7 | 1.9 ± 2.3 | 1.2 ± 0.8 | 1.4 ± 0.7 | +0.35(-0.84 to 1.54) | 0.77 |
Table 2:Changes in ejection fraction, body mass index and LDL levels in yoga and control groups after post-CABG rehabilitation, from [13]
| Baseline | 6th week | 1 year | ||||
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Wilcoxon p value | Mean ± SD | Wilcoxon p value | ||
| EF | Yoga | 52.22 ± 6.69 | 54.58 ± 5.8 | 0.001 | 55.91 ± 5.21 | 0.001 |
| Control | 53.39 ± .14 | 53.85 ± 6.33 | 0.001 | 54.12 ± 6.84 | 0.001 | |
| BMI (kg/m²) | Yoga | 26.76 ± 3.24 | 23.93 ± 2.56 | 0.001 | ||
| Control | 25.22 ± 3.15 | 24.93 ± 3.46 | ||||
| LDL > 100 | Yoga | 122.52 ± 2.60 | 91.38 ± 43.04 | 0.01 | ||
| Control | 114.67 ± 13.76 | 125.20 ± 33.87 | ||||
| LDL < 100 | Yoga | 66.54 ± 19.75 | 92.19 ± 28.58 | 0.01 | ||
| Control | 69.27 ± 17.21 | 91.15 ± 29.57 | ||||
Table 3:Cardiopulmonary exercise testing results from [21], * p<0.05 vs controls.
| Exercise training | Dance | Control | ||||
|---|---|---|---|---|---|---|
| Entry | 8 wk | Entry | 8 wk | Entry | 8 wk | |
| Peak V02 (ml/kg/min) | 16.5 ± 4.5 | 19.6 ± 4.5* | 16.8 ± 5.0 | 19.5 ± 5.0* | 16.1 ± 4.5 | 15.8 ± 4.5 |
| V02 AT (ml/kg/min) | 9.8 ± 3.2 | 11.9 ± 3.0 * | 9.9 ± 3.4 | 11.6 ± 3.3 * | 9.6 ± 3.0 | 9.4 ± 3.0 |
| VE/VC02 slope | 39.5 ± 11 | 31.8 ± 12 * | 38.8 ± 12 | 32.5 ± 12* | 39.1 ± 13 | 38.9 ± 1.1 |
| V02/W slope | 8.3 ± 1.5 | 9.5 ± 1.3 * | 8.1 ± 1.3 | 9.4 ± 1.1 * | 8.4 ± 1.1 | 8.3 ± 1.1 |
| Peak O2 pulse, ml beat | 10.5 ± 1.8 | 12.3 ± 1.8 * | 10.7 ± 1.7 | 12.6 ± 1.7 * | 10.2 ± 1.6 | 10.5 ± 1.6 |
Table 4:Review of Physical activities for cardiac rehabilitation for primary and secondary end-points.
| Primary end-point | Secondary end-points | |
|---|---|---|
| Tai Chi [12] | - (V02) | + (QOL MHFLQ, 6 min walk test, BNP levels |
| Yoga [13,14] | + (LVEF) ______________________________ - : MACE + : Coprimay outcome EQ-VAS score | + (BMI, lipid profile, QOL questionnaires*) ____________________________ + (reintegration to normal living index) |
| Waltz dance [21] | + V02 | + (MHFLQ, NYHA) |
MHFLQ : Minnesota Living with Heart failure questionnaire; LVEF Left ventricular ejection fraction; BMI : body mass index; QOL questionnaires=: HADS anxiety (p=0.001); HADS-depression (p=0.001); PSS (p=0.001) and PANAS-negative (p=0.003); MACE : major cardiac events; EQ-VAS score self-rated health (visual analogue scale EQ-5D-SL); NYHA New York Heart Association
Conflict of Interests
No Conflict of Interest.
References
1. Lawler PR, Filion KB, Eisenberg MJ. Efficacy of exercise-based cardiac rehabilitation post-myocardial infarction: A systematic review and meta-analysis of randomized controlled trials. Am Heart J. 2011;162.
2. Dugmore LD, Tipson RJ, Phillips MH, et al. Changes in cardiorespiratory fitness, psychological wellbeing, quality of life, and vocational status following a 12 month cardiac exercise rehabilitation programme. Heart. 1999;81:359‑66.
3. Taylor RS, Long L, Mordi IR, et al. Exercise-Based Rehabilitation for Heart Failure: Cochrane Systematic Review, Meta-Analysis, and Trial Sequential Analysis. JACC Hear Fail. 2019;7.
4. Taylor RS, Walker S, Ciani O, et al. Exercise-based cardiac rehabilitation for chronic heart failure: The EXTRAMATCH II individual participant data meta-analysis. Health Technol Assess (Rockv) Published Online First: 2019.
5. Ponikowski P, Voors A. 2016 Esc guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European society of cardiology (ESC): Developed with the special contribution . Russ J Cardiol. 2017.
6. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure. J Am Coll Cardiol. 2013; 62.
7. Jackson L, Leclerc J, Erskine Y, et al. Getting the most out of cardiac rehabilitation: A review of referral and adherence predictors. Heart. 2005.
8. Price KJ, Gordon BA, Bird SR, et al. A review of guidelines for cardiac rehabilitation exercise programmes: Is there an international consensus? Eur J Prev Cardiol. 2016; 23:1715‑33.
Piepoli MF, Corra U, Benzer W, et al. Secondary prevention through cardiac rehabilitation: from knowledge to implementation. A position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation. Eur J Cardiovasc Prev Rehabil. 2010;17:1‑17.
10. Gayda M, Ribeiro PAB, Juneau M, et al. Comparison of Different Forms of Exercise Training in Patients With Cardiac Disease: Where Does High-Intensity Interval Training Fit? Can J Cardiol. 2016; 32.
11. Ribeiro PAB, Boidin M, Juneau M, et al. High-intensity interval training in patients with coronary heart disease: Prescription models and perspectives. Ann Phys Rehabil Med. 2017; 60.
12. Yeh GY, Wood MJ, Lorell BH, et al. Effects of Tai Chi mind-body movement therapy on functional status and exercise capacity in patients with chronic heart failure: A randomized controlled trial. Am J Med Published Online First. 2004.
13. Raghuram N, Parachuri VR, Swarnagowri M V, et al. Yoga based cardiac rehabilitation after coronary artery bypass surgery: One-year results on LVEF, lipid profile and psychological states - A randomized controlled study. Indian Heart J Published Online First. 2014.
14. Prabhakaran D, Chandrasekaran AM, Singh K, et al. Yoga-Based Cardiac Rehabilitation After Acute Myocardial Infarction: A Randomized Trial. J Am Coll Cardiol. 2020;75:1551‑61.
15. Christa E, Srivastava P, Chandran DS, et al. Effect of Yoga-Based Cardiac Rehabilitation on Heart Rate Variability: Randomized Controlled Trial in Patients Post-MI. Int J Yoga Therap. 2019;29.
16. Zou L, Sasaki J, Wei G-X, et al. Effects of Mind–Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J Clin Med 2018;7.
17. Hendriks T, De Jong J, Cramer H. The effects of yoga on positive mental health among healthy adults: A systematic review and meta-analysis. J Altern Complement Med. 2017;2 3.
18. Reddy P, Dias I, Holland C, et al. Walking football as sustainable exercise for older adults–A pilot investigation. Eur J Sport Sci Published Online First. 2017.
19. Arnold JT, Bruce-Low S, Sammut L. The impact of 12 weeks walking football on health and fitness in males over 50 years of age. BMJ Open Sport Exerc Med Published Online First. 2015.
20. Rawstorn JC, Gant N, Direito A, et al. Telehealth exercise-based cardiac rehabilitation: A systematic review and meta-analysis. Heart. 2016.
21. Belardinelli R, Lacalaprice F, Ventrella C, et al. Waltz dancing in patients with chronic heart failure: new form of exercise training. Circ Heart Fail Published Online First: 2008.
Received: Feb 02, 2021;
Accepted: Feb 12, 2021;
Published: March 02, 2021.
To cite this article : Philippe DUC, Christine IM, Claude AM, et.al. What Physical Activities can be Recommended in Cardiac Rehabilitation Centers? British Journal of Heart Diseases. 2020; 3:1.
© Philippe DUC , et.al. 2021.